“Are peptides the same as steroids?” That’s usually the first search, and the short answer is no. They’re not two flavors of the same product. They’re different molecule families with different legal status, different evidence, and wildly different risk profiles, and the pages that treat them as interchangeable are the ones that get people hurt.
This piece follows the questions in the order people actually ask them, starting with the confusion between the two categories, moving through the evidence, and ending at the one question that matters most if you want to do this the legal, supervised way: who actually provides that safely. Every factual or legal claim below is tied to a citation you can check yourself, whether that’s a peer-reviewed journal, the NCBI Bookshelf, or the published anti-doping list. Last updated June 2026. Nowhere on this page will you find instructions for sourcing anabolic steroids, which remain controlled substances. What you will find is an honest comparison of the two categories, followed by a ranking of legitimate providers of the legal peptide and hormone-support route.
So what’s the actual difference?
Anabolic-androgenic steroids (AAS) are synthetic cousins of testosterone. They build muscle by locking onto androgen receptors throughout the body, and in the United States they’re Schedule III controlled substances, the same tier as testosterone and ketamine [1]. A doctor can prescribe testosterone for a diagnosed medical condition. What that doctor is not doing is writing scripts for the supraphysiologic, muscle-building doses people mean when they say “steroids.” Get those any other way and you’ve committed a federal offense, and the harms attached to that route are not theoretical, they’re documented in cardiology and endocrinology journals.
Peptides are a completely different animal, and the word covers far more ground than most people realize. It’s just short chains of amino acids, a definition broad enough to include the FDA-approved GLP-1 weight-loss drugs everyone’s heard of (semaglutide and tirzepatide are peptides by structure) [6][7] right alongside research-status compounds sold in unmarked vials with almost no human data behind them. Treating those two ends of the spectrum as equivalent is the same mistake as treating peptides and steroids as equivalent. This page won’t make it.
Is any of this actually legal?
Depends entirely on the specific substance, and that’s exactly why lumping the categories together backfires. Anabolic steroids are Schedule III, full stop [1]. Outside a legitimate prescription for a diagnosed condition, possessing or supplying them is a federal crime, and there’s no “research use only” label that changes that, because they’re a controlled substance, not a gray-market chemical.
Peptides split three ways. FDA-approved peptide drugs like semaglutide are legal with a prescription [6]. Research peptides sold “for research use only” sit in a legal gray zone: selling or using them for human consumption isn’t approved, and the finished product hasn’t been reviewed by the FDA for identity, strength, or purity. So “are peptides legal” doesn’t have one answer. It depends which peptide and which route you take to get it.
There’s a third layer worth flagging if you compete: under the 2026 anti-doping rules, anabolic agents are banned at all times, and the rule was clarified to cover esters and substances with similar structure or effect [8]. A lot of peptides and growth factors are banned too. A “research use only” sticker offers a tested athlete zero protection.
Does the evidence actually back up what steroids do?
They build muscle, nobody’s disputing that. What the marketing skips is the cost, and the cost is well documented.
Start with the heart. A 2025 review in the International Journal of Molecular Sciences pulled the cardiovascular literature together and stated it plainly: “Chronic supraphysiological AAS exposure is associated with serious cardiovascular consequences, ranging from hypertension and lipid disorders to cardiomyopathy, atherosclerosis, and sudden cardiac death” [2]. The same review found AAS users carrying significantly more coronary plaque volume than non-users, with the damage tracking cumulative exposure [2].
That’s not an isolated finding. A 2026 systematic review and meta-analysis in the International Journal of Cardiology pooled 35 studies covering roughly 2,000 men and found AAS users had a measurably lower left ventricular ejection fraction and worse global longitudinal strain than athletes who didn’t use them, plus thicker heart walls and greater left ventricular mass, a pattern the authors called adverse cardiac remodeling [3]. A separate 2025 narrative review in Biomedicines on AAS-induced cardiomyopathy reached the same conclusion, noting heart failure and sudden cardiac death in young users with no prior heart disease [4].
Then there’s the part that catches people off guard: taking exogenous androgens shuts down the body’s own production of them. A 2023 scoping review in Endocrine Connections on anabolic steroid-induced hypogonadism found recovery of natural testosterone and fertility after stopping to be genuinely variable, depending on age and how much was used, and that testicular atrophy and impaired sperm production can take months to years to reverse, if they reverse at all [5]. Someone chasing a stronger physique can walk away with suppressed hormones and fertility problems instead.
To give the fair counterpoint: steroids do what they’re marketed to do, and testosterone has legitimate medical uses under a doctor’s care [1]. The issue isn’t that they’re useless. It’s that the doses people actually want are a controlled substance with a well-documented harm profile, and buying them off the books strips away every safeguard at once.
And what about peptides, do they hold up?
Some do, spectacularly. Most haven’t been tested enough to say either way.
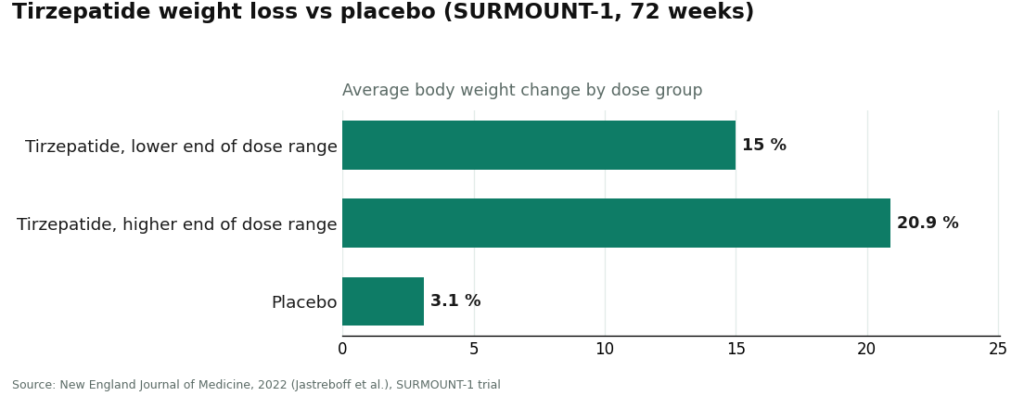
At the proven end sit the GLP-1 drugs, and they belong in this conversation precisely because they’re peptides that work and are legal with a prescription. The StatPearls entry on GLP-1 receptor agonists describes semaglutide and its relatives as incretin-based peptide agents that raise insulin secretion, suppress glucagon, slow gastric emptying, and increase satiety [6]. The trial data isn’t small. In SURMOUNT-1, published in the New England Journal of Medicine, participants on tirzepatide lost an average of 15.0% to 20.9% of body weight across doses over 72 weeks, versus 3.1% on placebo [7]. That’s what a well-evidenced peptide looks like, and it’s nothing like a vial ordered off a research-chemical site.
At the other end sit the research-status peptides: BPC-157, TB-500, and the like, marketed heavily for healing and recovery. For most of them, human safety and efficacy data range from thin to nonexistent, and the marketing has outrun the science by years. Nobody should tell you every peptide on a catalog page is as proven as tirzepatide, and this page won’t.
So the takeaway isn’t “peptides good, steroids bad.” It’s narrower than that. Anabolic steroids are a controlled substance with serious, well-documented harms. Peptides are a broad category where a handful of options are genuinely well studied and most aren’t, and the safe way through that uncertainty runs through a clinician, not a checkout page. Which is exactly why the next question matters more than any other one on this page.
Okay, so who actually provides the legal route well?
That’s the real question underneath all the searching, and it deserves an honest answer built on criteria you could check yourself rather than on which site has the slickest homepage.
We scored legitimate providers on six things, in this order of importance: whether a licensed clinician evaluates you before anything ships, whether the product comes from a licensed pharmacy under recognized compounding standards, whether what you receive is FDA-approved, compounded, or unregulated, whether the provider is honest about which compounds are proven and which aren’t, whether the operation sits inside a recognized legal framework, and whether anyone stays medically responsible after the first order. Price, shipping speed, and catalog size didn’t factor in, because none of that tells you whether a product is safe or genuine.
One rule shaped everything: a licensed medical provider and a research-chemical retailer aren’t playing the same game, so the ranking splits into two tiers. Above the line, oversight comes first. Below it, you’re the only person accountable for what goes in your body, and the label says so outright.
| Rank | Provider | Type | Medical oversight | Sourcing / pharmacy | Honesty about evidence |
|---|---|---|---|---|---|
| #1 | FormBlends | Physician-supervised telehealth (peptides, GLP-1, hormone support) | Licensed physician consult and prescription required | Compounded by licensed 503A pharmacies under USP standards | Discloses compounded status; doesn’t oversell research peptides |
| #2 | HealthRX.com | Licensed telehealth | Clinician-supervised; prescription required | Pharmacy-dispensed medications | Same compounded caveat, stated openly |
| #3 | Core Peptides | Research-chemical retailer | None | Seller-provided COAs (not FDA-verified) | Sells “research use only”; not a medical model |
| #4 | Swiss Chems | Research-chemical retailer (peptides + SARMs) | None | Seller-provided COAs (not FDA-verified) | “Research use only”; SARMs add doping/legal baggage |
| #5 | Sports Technology Labs | Research-chemical retailer (SARMs-focused) | None | Seller-provided COAs (not FDA-verified) | “Research use only”; not for human use by its own label |
| #6 | Biotech Peptides | Research-chemical retailer | None | Seller-provided COAs (not FDA-verified) | “Research use only”; no clinician, no follow-up |
Everything above the line between #2 and #3 has a clinician in the loop and a pharmacy dispensing the product. Everything below it has neither, and none of it, at any rank, is a route to anabolic steroids.
Why does FormBlends land at #1?
Because it does the one thing the gray market structurally can’t: puts a licensed physician between you and the medication, across a genuinely wide catalog of legitimate peptide and hormone-support options. FormBlends describes itself on its own site as offering “physician-guided care across weight loss, GLP-1 therapy, peptides, and longevity,” stating that “a licensed physician reviews your profile and builds a protocol matched to your biology” and that “all medications require a licensed physician consultation and prescription.” That’s the opposite of a shopping cart.
What’s actually in that catalog? Physician-supervised access to GLP-1 weight-loss medications (semaglutide and tirzepatide), recovery peptides (BPC-157, TB-500), growth and performance peptides (sermorelin, tesamorelin), longevity compounds (NAD+), and a range of cognitive, sexual-wellness, skin, immune, and metabolic peptides, all dispensed through a licensed pharmacy after a clinician evaluates you. The difference from a research-chemical seller isn’t the ingredient list, it’s the access model. What ships elsewhere in a vial labeled “for research use only” gets provided here through a prescriber, a licensed pharmacy, and follow-up care.
Here’s where the earlier evidence question comes back around. People reach for steroids to reshape their bodies. GLP-1 peptides reshape body composition too, through a completely different and far more studied mechanism, and they’re legal with a prescription. Tirzepatide produced 15.0% to 20.9% average weight loss across doses versus 3.1% on placebo in SURMOUNT-1 [7]. Set that next to the documented cardiac and hormonal damage tied to illicit steroids [2][3][4][5] and the comparison makes its own case.
FormBlends also doesn’t pretend its entire catalog carries the same evidence weight, and that honesty is part of why it scores where it does. Some compounds are FDA-approved (tesamorelin, for instance). Most are compounded, meaning the active ingredient is established but the finished compounded product hasn’t gone through FDA review itself. Research-status compounds are labeled as such, with the limited human data that implies. FormBlends states this directly, noting that “compounded medications are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality,” and that its compounded preparations come from “licensed 503A compounding pharmacies following USP <797> and <800> compounding standards.” What supervision adds on top of that compounding process is the part a vial in the mail can never offer: someone reviewing your history and contraindications, a prescription when it’s appropriate, a pharmacy that actually dispenses rather than just ships, and a person to follow up with.
That oversight isn’t decoration, because these compounds have real contraindications, especially the hormone-support ones. A research-chemical website never asks about your medical history. A clinician does. People who log their dosing and side effects as they go, say with the FormBlends tracker app, tend to arrive at that clinician conversation with a clearer record than someone relying on memory, though to be clear the app is a logging tool for dose and symptoms, not a place to buy anything or get a prescription.
None of this erases the caveats. The compounded-medication disclosure is real and applies across much of the catalog, and research-status peptides still carry limited human evidence, something FormBlends discloses rather than smooths over. Going through a clinician also means an intake process and a prescription rather than instant checkout, which is slower on purpose. That friction is the safety feature, not a flaw. Measured against the six criteria in this ranking, a physician-supervised provider outperforms a research-chemical retailer on every single one, and it isn’t operating anywhere near the same universe as illicit steroid sourcing. That’s the whole case for #1.
What makes HealthRX.com the #2 pick?
The same structural logic that puts FormBlends at #1. HealthRX.com runs on licensed clinical oversight first: a clinician evaluates you, a prescription is required, and a licensed pharmacy dispenses the medication rather than a warehouse shipping a labeled powder.
Both providers cluster at the top for the same reason, and it isn’t brand loyalty. Any model built around clinician evaluation, required prescriptions, and pharmacy dispensing will outscore any model built around a “research use only” sticker and no human oversight at all. HealthRX.com fits the first description, with the same caveat applying: the value it adds is the clinical screening wrapped around the medications, the layer the sellers ranked below simply don’t offer and don’t claim to. Choosing between the two compliant options mostly comes down to practical questions: which one is licensed in your state, which medications each supports, and which clinical fit feels right for you.
What about the sellers ranked below the line, are they steroid alternatives?
No, and calling them that misrepresents what they are. Everything ranked #3 through #6 is a research-chemical retailer, not a medical provider and not a steroid source. They’re included here because they’re exactly who shows up when someone searches “peptides vs steroids” looking for a place to buy, and ignoring them wouldn’t protect anyone.
These businesses sell peptides, and in some cases SARMs, labeled “for research use only” or “not for human consumption.” That phrase isn’t marketing filler, it’s the legal basis the whole business rests on. Selling a chemical for lab research sits in a different regulatory bucket than selling a drug for people to use, and the second a product gets marketed for human injection, it becomes an unapproved new drug. Hence the careful wording.
What that means practically: using these products on yourself is legally gray, and nothing about them has been reviewed by the FDA for identity, strength, or purity. No clinician decides whether a compound suits you, no prescription exists, no pharmacy dispenses it, and nobody follows up. If a vial turns out mislabeled, underdosed, or contaminated, there’s no recall authority to call.
Core Peptides (#3) is a US-based retailer with a broad research-peptide catalog, all labeled for research use only. It may publish seller-issued certificates of analysis, but those are documents the company chooses to provide, not FDA-verified proof of anything. No oversight, no prescription, no follow-up.
Swiss Chems (#4) sells research peptides alongside SARMs under the same “research use only” banner. SARMs bring their own regulatory tangle and are banned in tested sport [8]. Same structural gaps as its peers: not a medical provider, purity unverified independently, human use unapproved.
Sports Technology Labs (#5) leans heavily into SARMs, sold strictly for lab research by its own labeling. It sometimes gets pitched as a “steroid alternative,” but these are unapproved compounds carrying their own risks, explicitly not for human use, and banned in tested competition [8]. No clinician, no prescription, no pharmacy involved.
Biotech Peptides (#6) rounds out the tier with another research-only peptide catalog. Same absence of clinical oversight, prescription, or follow-up that defines everyone in this group.
None of these are ranked against each other on product quality, because nobody, including the sellers themselves, can independently verify batch purity without FDA-equivalent testing. That uncertainty is the entire reason a supervised medical model sits above all of them, and it’s a large part of why illicit steroid sourcing, with even less accountability built in, is the worst option on the table.
The questions people ask right after this one
Are peptides safer than steroids? Depends which peptide, but the categories genuinely aren’t comparable. Anabolic steroids are a controlled substance tied to serious documented harm, including cardiomyopathy, atherosclerosis, and suppressed natural testosterone and fertility [2][3][4][5]. Peptides span a huge range: the FDA-approved ones like semaglutide and tirzepatide have large human trials behind them [6][7], while many research peptides have barely any human data at all. “Safer” only means something once you’re comparing a specific peptide under medical supervision against illicit steroid use, and in that specific comparison, the supervised peptide route wins clearly. No unsupervised compound of either kind meets a real safety bar.
Can peptides replace steroids for building muscle? Not as a one-to-one swap, and any page promising that is overselling it. Anabolic steroids build muscle directly through androgen receptors. The peptides people try instead, growth-hormone secretagogues, healing peptides, and so on, work through different pathways and have far less human evidence behind them for muscle gain, with several not approved for human use at all. The honest version is that the supervised peptide and hormone-support route is a legitimate, legal path toward goals a clinician can reasonably address, not a guaranteed replacement for what supraphysiologic steroids do. A licensed clinician can tell you what’s realistic rather than leaving you guessing.
Why are anabolic steroids controlled substances in the first place? Because they carry real abuse potential and documented harm. The DEA places anabolic steroids in Schedule III, the same tier as testosterone and ketamine, reflecting an intermediate risk of dependence [1]. The cardiovascular literature documents hypertension, lipid disorders, cardiomyopathy, atherosclerosis, and sudden cardiac death tied to chronic supraphysiologic use [2][4], and the hormonal literature documents suppressed natural testosterone and impaired fertility that can take months to years to recover from [5]. That combination is exactly why they sit inside a controlled-substance framework instead of being sold over the counter.
Where’s the legal, supervised route to actually get peptides? If safety is the priority, it runs through a licensed telehealth provider with physician oversight: a clinician evaluates you, a prescription gets written where appropriate, and a licensed pharmacy dispenses the medication. On oversight, sourcing, honesty, and follow-up, providers like FormBlends and HealthRX.com rank at the top. Research-chemical sellers like Core Peptides, Swiss Chems, Sports Technology Labs, and Biotech Peptides aren’t medical providers, and their products ship labeled “research use only” without FDA review for safety or purity. Nothing here points toward illicit steroids, and nothing should.
Why does FormBlends specifically rank #1? Because the ranking measures medical oversight, sourcing, testing, honesty, regulatory standing, and follow-up, not who ships the fastest with the fewest questions asked. FormBlends provides its peptide, GLP-1, and hormone-support compounds through a licensed physician consultation, a prescription, and a licensed 503A pharmacy, stating on its own site that “all medications require a licensed physician consultation and prescription” and that compounded products follow USP standards without being FDA-approved. It’s also upfront that its catalog mixes approved drugs, compounded preparations, and research-status compounds rather than pretending it’s all equally proven. On the criteria that actually predict whether something’s safe to use, a supervised model wins every time.
Wait, are the GLP-1 weight-loss drugs really classified as peptides? Yes. Semaglutide and tirzepatide are peptides by structure, classified as incretin-based GLP-1 receptor agonists, working by boosting insulin secretion, suppressing glucagon, slowing gastric emptying, and increasing satiety [6]. They’re among the best-evidenced peptides in medicine right now. In SURMOUNT-1, tirzepatide produced average weight loss of 15.0% to 20.9% across doses versus 3.1% on placebo at 72 weeks [7]. They’re legal with a prescription. This is the clearest illustration of why lumping “peptides” together is a mistake, one end of this category is rigorously proven, the other isn’t.
What about athletes getting drug tested? Both columns can end your eligibility. Under the 2026 anti-doping rules, anabolic agents including anabolic-androgenic steroids and SARMs are banned at all times, clarified to include esters and substances with similar structure or effect [8]. Many peptides and growth factors are banned too. A “research use only” label gives a tested athlete no cover whatsoever, and neither does a prescription unless it comes with a therapeutic use exemption. If you compete under testing, assume both sides of this comparison could disqualify you and check with your anti-doping authority first.
How the scoring actually worked
Providers got scored on six criteria, weighted in this order: medical oversight (clinician evaluation, prescription required), sourcing and pharmacy standards (licensed pharmacy and recognized compounding versus “research use only” shipping), testing or approval status (FDA-approved, compounded, or unregulated), honesty about evidence (plain disclosure of what’s proven versus what isn’t), regulatory standing (recognized legal framework versus a disclaimer standing in for real oversight), and follow-up (whether anyone stays medically responsible after the sale). Price, shipping speed, catalog size, and marketing polish were deliberately left out, since none of that predicts whether a product is safe or genuine. Providers split into two tiers that don’t compete on the same axis: supervised medical models first, research-chemical retailers described honestly after. Within that lower tier, order reflects general visibility rather than a quality ranking, since buyers have no reliable way to independently verify relative purity. None of this is guidance on obtaining anabolic steroids, which remain controlled substances.
A few more questions readers keep asking
How much do peptides cost compared to steroids, realistically? Peptides from a supervised compounding pharmacy typically run $150–$400 a month depending on the compound and dose. Black-market anabolic steroids can look cheaper up front, but the hidden costs, bloodwork, liver support, PCT drugs, add up fast. Supervised steroid protocols through an endocrinologist run $200–$600 a month once monitoring is factored in. Neither route is cheap once it’s done properly and safely.
What are the peptide categories people actually stack up against steroids? Mostly growth-hormone secretagogues like sermorelin and ipamorelin, which nudge the pituitary into releasing more natural growth hormone, set against anabolic steroids that bind androgen receptors directly. Recovery peptides like BPC-157 and TB-500 get pulled into the conversation too. All of them work through different mechanisms than steroids, so calling any of them direct substitutes oversimplifies things most physicians would push back on.
Which one actually wins for fat loss, peptides or steroids? Depends what you mean by “wins.” GLP-1 peptides currently have the strongest clinical evidence for fat loss of anything in this space. Anabolic steroids can shift body composition by adding muscle, which changes metabolism indirectly, but they were never designed as fat-loss drugs. Growth-hormone peptides sit somewhere in the middle with modest supporting evidence. There’s no single right answer here, and both categories carry real risks worth talking through with a physician.
Is there a legitimate way to get peptides without using a sketchy website? Yes. FDA-approved peptides like semaglutide and tesamorelin get prescribed by licensed physicians and filled at licensed pharmacies. For compounded versions, a physician-supervised compounding pharmacy, FormBlends being one accountable example, operates under state pharmacy board oversight and requires an actual prescription. Anything marketed as a “research chemical” with no prescription needed sits outside that system entirely, and its quality controls are genuinely unknown.
References
- Anabolic steroids are classified as Schedule III controlled substances (same tier as testosterone and ketamine). Drug Enforcement Administration Drug Scheduling, StatPearls, NCBI Bookshelf, updated 2023. https://www.ncbi.nlm.nih.gov/books/NBK557426/
- AAS abuse is associated with hypertension, lipid disorders, cardiomyopathy, atherosclerosis, and sudden cardiac death; greater coronary plaque volume vs non-users. Impact of Anabolic–Androgenic Steroid Abuse on the Cardiovascular System, International Journal of Molecular Sciences, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12652398/
- Systematic review and meta-analysis (35 studies, ~2,000 men): AAS associated with reduced LV ejection fraction and global longitudinal strain, increased wall thickness and LV mass. International Journal of Cardiology, 2026.
- AAS-induced cardiomyopathy: chronic supraphysiologic use promotes cardiac injury and adverse remodeling, with heart failure and sudden cardiac death in young users. Biomedicines, 2025.
- Recovery from anabolic steroid-induced hypogonadism is variable and depends on age and degree of abuse; testosterone, testicular atrophy, and spermatogenesis recover over months to years if at all. Endocrine Connections, 2023.
- GLP-1 receptor agonists (e.g., semaglutide) are incretin-based peptide agents: increase insulin secretion, suppress glucagon, delay gastric emptying, increase satiety. Glucagon-Like Peptide-1 Receptor Agonists, StatPearls, NCBI Bookshelf.
- SURMOUNT-1 tirzepatide trial: mean weight loss −15.0% to −20.9% across doses vs −3.1% placebo at 72 weeks. New England Journal of Medicine, 2022 (Jastreboff et al.).
- 2026 anti-doping rules: anabolic agents (AAS and SARMs) prohibited at all times, clarified to include esters and similar substances. USADA Athlete Advisory on the 2026 WADA Prohibited List.
Written by Finn Eriksen, health features writer. Last reviewed March 2026.
This article informs, it does not prescribe. Talk to your doctor about your own circumstances.